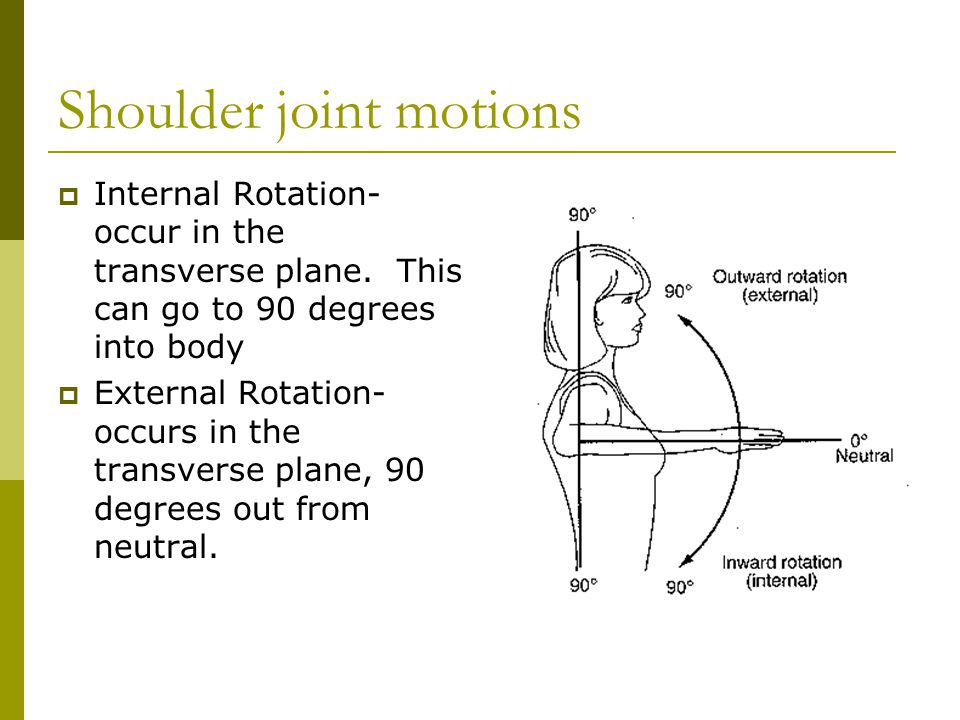
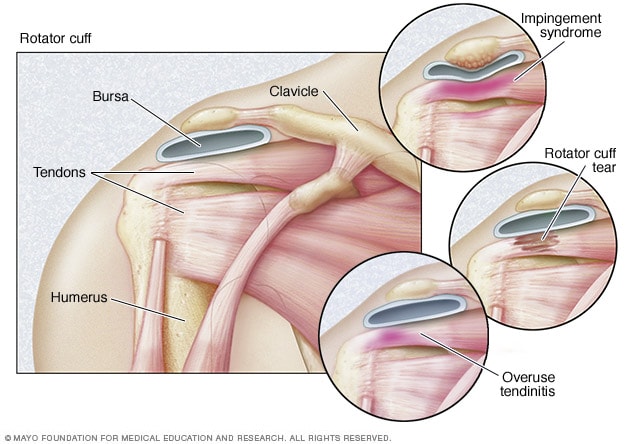
A bit confused by this. The test you show (2nd image above) appears to test ISR (and perhaps other shoulder function). However, the Infraspinatus is employed for ESR. Puzzling. It it possible that it has an effect on ISR? It is the
Subscapularis that is the rotator muscle employed for ISR.
Along with the (lateral) deltoid, the Supraspinatus is utilized for shoulder abduction. I believe that the anterior deltoid is involved in shoulder flexion and posterior deltoid for extension. Not sure which rotator muscles might assist in flexion and extension.
@RogueFLIP or anyone else in the know... do you have a better understanding of all this?
You're getting confused because you're trying to separate each individual rotator cuff muscle into their specific action, where as in reality it's not like one shuts off and another one turns on as you go through motions of ESR and ISR.
Also remember that muscles can contract concentrically (shortening) & eccentrically (lengthening). So while yes, the main function of the infraspinatus is to concentrically contract during ESR, it will contract eccentrically during ISR. So yes it can be affected and affect ISR.
@RaulSJ
But my own hypothesis for Raul SJ issues is that it's more of a postural issue that is mainly contributing to the problem.
Judging from your pic, look at your left arm. It's internally rotated at the humerus bc your palm is facing the picture. If your right palm does the same resting at your side, well then your R humerus is also rotating inwards, which might be causing a minor impingement to the front of the shoulder. Normally when your arms are resting at your side, your thumbs should be pointing forward. That's the neutral position.
Second, the tops of your shoulder by your scapula look very rounded, like they're pitching forward; now it could just be the lighting and shadows.....but if I'm right, then this posture also will add to closing the joint space of the front of your shoulder....another minor factor to possible impingement.
Raul SJ, exaggerate some forward posture.....stand up, slouch head and shoulders forward, turn your arms inward so your palms face behind you and try to raise your arms to point to the ceiling. Notice the feel.
Now, stand up straight, nice and tall, arms with your thumbs facing forward and raise your arms to point to the ceiling. Notice this feel. Which one feels easier and more fluid?
So basically, if you've been in that forward rounded posture where everything is tight in the front of you (internal rotators), guess what has to work extra hard to compensate? The opposite (external rotators). So then you wonder why you've developed issues.
I've utterly oversimplified things mate.....
Something to consider......I'm off to bed.....
![52-image[11].png](http://1h6wllf3f4qfut1832zlo21e-wpengine.netdna-ssl.com/wp-content/uploads/blogger/52-image[11].png)





![Range-of-Motion[1].jpg](https://www.sghs.org/images/Range-of-Motion[1].jpg)