Background.
The OP posted a question addressed to me because: 1) he had posted video of his serve earlier and I had said I thought that his upper arm looked too high and he should look into it. 2) he was concerned and we had discussed it in other threads. 3) in this thread I thought that he had a Waiter's Tray technique. 4) Available Information on how high the arm should be to minimize the risk of impingement applies to the high level serving technique. I don't know about other techniques such as the Waiter's Tray.
Todd Ellenbecker produced a video called "Rotator Cuff Injury" that used to be available free on Youtube. I referenced it many times on the forum. It is no longer available free. It is still available through Tennis Resources by joining (one month memberships are available, the lowest cost option). It may also be for sale from Tennis Resources but I don't know. ? It was the best thing I've seen to explain shoulder impingement during the tennis serve and I recommend it. From Ellenbecker's discussion, I believe that it applies to the high level serving technique involving internal shoulder rotation and it is not clear if or how it applies to other techniques. A majority of active tennis players do not use a high level serving technique.
Better ATP servers are examples of best practice. Videos and pictures taken from specific camera angles are the best references available for shoulder abduction or other useful angles. But they don't measure angles accurately because the camera image is only a 2D view of 3D space.
Anatomy references.
http://healthfixit.com/sternum/
Anatomy video detailing the sternum, clavicle and scapula. See the sternoclavicular joint and scapulothoracic joint.
---------------------------------------------------------------------------------------------------------------------------
When the arm is raised high to impact the ball on the serve there are issues on how to measure "shoulder abduction" angle or other useful angles. I have never had a clear idea of how to accurately measure 'shoulder abduction' for this issue either from the Ellenbecker video or other sources. It seems there are working definitions of shoulder abduction that involve more than just the glenohumeral joint. These working definitions for shoulder abduction may include the sternoclavicular joint angle and scapulothoracic joint angle in addition to the glenohumeral joint angle.
What goes on during a serve to cause impingement seems to be somewhat uncertain but there are reasonable descriptions of what might cause impingement.
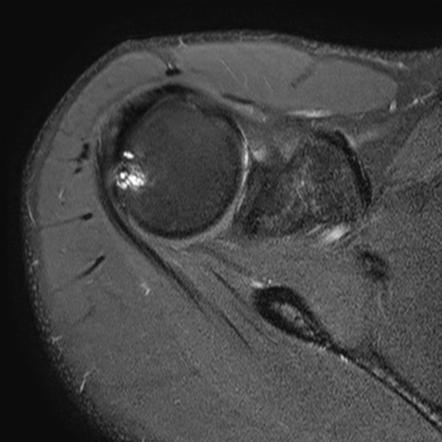
Shoulder impingement, as I understand it, directly involves just two bones, the humerus and the scapula. These two bones meet at the glenoid fossa, literally forming the one and only 'shoulder joint', the glenohumeral joint. The second part of the scapula bone involved in impingement is the acromion. The angle that is needed for impingement is the angle at which the humerus is too close to the acromion. The humerus also has boney high points that increase impingement when the humerus is unfavorably rotated. Needs more research on the issue.
We need a cook book type instruction to estimate the risk of impingement for the high level technique of the tennis serve.
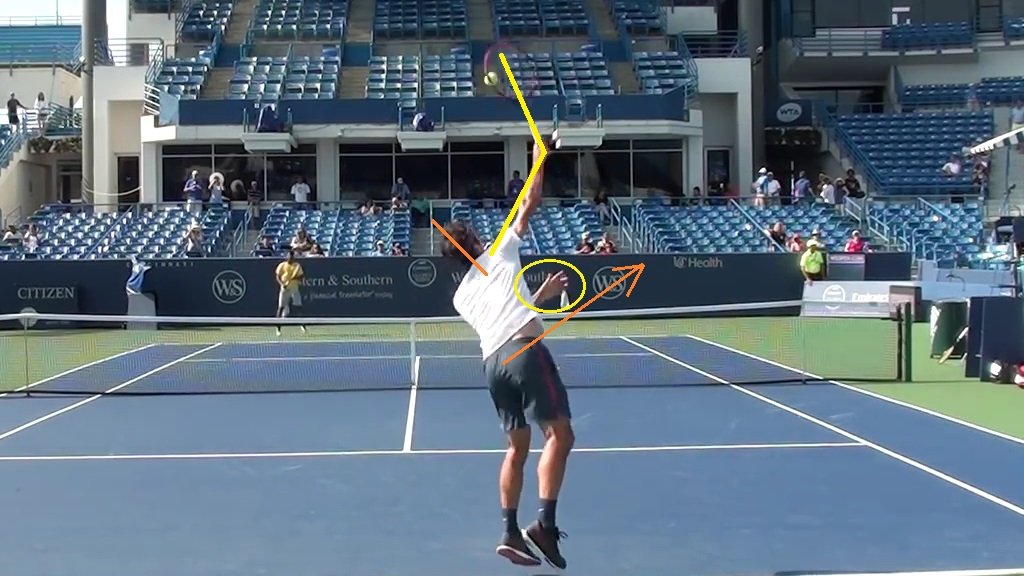
I compare the upper arm orientation to the shoulder by: 1) drawing a line between the two shoulders, 2) extending that line and 3) measuring the angular orientation of the upper arm to that extended line. That usually produces an angle such as 10 to 30 d up. These lines are what David Whiteside described and I believe I have seen these lines described elsewhere for the tennis serve. But shoulder abduction for this issue seems to me less and less a useful angle for the average tennis player to use.
Reasons that I like using the
extended line of the shoulders and the upper arm (humerus):
1) I am much, much more familiar with angles up to 90 d than I am with larger angles. For example, I know '45 d' very well but I have to think about 135 d. Therefore, I vote for using angles smaller than 90 d because they are much more familiar to the average person.
2) The angle of the upper arm to the extended line between the two shoulders is closely related to and similarly oriented to what the impingement risk is most likely related to - the upward angle of the humerus to the scapula/acromion.
3) We would like to see the orientation of the scapula but we can't see that in videos (maybe without a shirt?).
4) The locations of the left and right shoulders usually can be easily seen and estimated in videos.
5) Drawing a line between the two shoulders is not perfect because the right and left shoulders can be independently elevated. Each shoulder can be elevated up to 45 d and depressed down to 5 d. Although for a tennis serve, the two shoulders seem to be used in an alignment of one high and one low with the shoulder girdle is in a line. Drawing the shoulders line is a compromise to get a useful estimate. Needs more work.
6) The angle of the scapulothoracic and sternoclavicular joints have less influence when measuring from the shoulders line extended than measuring from a reference line on the thoracic chest. This issue needs more work.
7) I believe that 'shoulder abduction' as used for various purposes, such as clinical measurements and the tennis serve estimates, is not synonymous with the angle of the glenohumeral joint. In my opinion, the angle of the glenohumeral joint is the most important thing for impingement risk. I don't know if the angle of the glenohumeral joint itself has been defined. Were reference points on the scapula somehow used as a reference line? When the humerus gets too close to the acromion, impingement risk increases but we can't see how the scapula is oriented.
The shoulders line and upper arm angle seems to work pretty well.....
We need a cook book instruction for impingement risk.
Until then, look at the upper arm orientation of high level ATP servers in high speed videos using as near identical camera viewing angles as possible. I believe comparing shoulder angles to angles on high level serve works very well, but I'd hate to try to prove it.............
")

 youtube.com
youtube.com